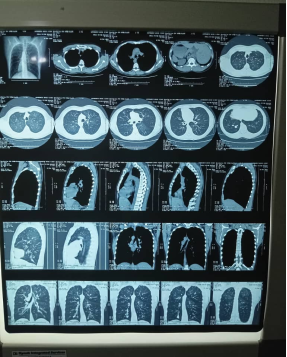
Background: Kartagener’s Syndrome (KS) is a rare autosomal recessive genetic disorder characterized by defects in the structure and function of cilia. It is a subset of primary ciliary dyskinesia (PCD) and is defined by a triad of chronic sinusitis, bronchiectasis, and situs inversus totalis. The condition often leads to infertility due to impaired sperm motility. Given its rarity and overlapping symptoms with other respiratory diseases, KS is frequently misdiagnosed. Case Presentation: Our client was a 40-year-old male who presented to the Rivers State University Teaching Hospital, Port Harcourt, Rivers State, South-south Nigeria with recurrent productive cough, rhinorrhea, exertional breathlessness, and wheezing—symptoms have been present since childhood. He had been managed for bronchial asthma at a peripheral center and also reported a history of primary infertility for six years. Clinical examination revealed respiratory distress, oxygen saturation of 87% on room air, and auscultatory findings of coarse crepitations and inspiratory rhonchi. Notably, cardiac auscultation localized heart sounds to the right side of the chest, raising suspicion of situs inversus. A chest computed tomography (CT) scan confirmed cystic bronchiectasis and situs inversus totalis, leading to a diagnosis of Kartagener’s Syndrome. Spirometry demonstrated an obstuctive ventilatory pattern with significantly reduced Forced Expiratory Volume in 1 second (FEV1), Forced Vital Capacity (FVC) and FEV1/FVC ratios. The patient was managed with antibiotics, bronchodilators, steroids, antihistamines, and chest physiotherapy. Educating and counseling the patient on disease condition, referred to psychotherapists/ Social support group. He remains under follow-up in the respiratory clinic for long-term care. Conclusion Kartagener’s Syndrome, though rare, has been reported globally (1–5). Due to symptom overlap with asthma and other chronic respiratory conditions, it is frequently underdiagnosed. Early recognition using clinical evaluation and imaging studies is crucial for appropriate management and improved patient outcomes.
| Published in | Central African Journal of Public Health (Volume 11, Issue 6) |
| DOI | 10.11648/j.cajph.20251106.16 |
| Page(s) | 381-384 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Primary Ciliary Dysfunction, Kartagener’s Syndrome, Clinical Presentation, Diagnosis, Management, Nigeria, Challenges
Indices | Predicted | Measured pre-bronchodilator | %Predicted | Measured post bronchodilator | %Predicted | ◇(Change) |
|---|---|---|---|---|---|---|
FEV1(L) | 3.2 | 1.60 | 50 | 2.0 | 63 | +0.4L (25%) |
FVC (L) | 4.0 | 3.2 | 80 | 3.5 | 88 | +0.3L (9%) |
FEV1/FVC (%) | 80.0 | 50.0 | - | 0.57 | - | +7% |
PEFR (L/s) | 8.0 | 4.5 | 56 | 5.8 | 72 | +1.3L/s (29%) |
FEF25-75%(L/s) | 3.5 | 1.1 | 31 | 1.7 | 49 | +0.6L/s (55%) |
Parameter | Result | Reference Range |
|---|---|---|
Volume | 2.5 | 1.5-5ml |
Appearance | Opalescent | Whitish, opaque |
PH | 7.4 | 7.2-8.0 |
Concentration | 8million/ml | 15-200million/ml |
Total sperm count | 20million | Million |
Motility (Progression count) | 10% | Greater than 40% |
Motility (Non-progressive) | 15% | Less than 10% |
Non-motile | 75% | Less than 40% |
Morphology | 2% | Greater than 4% (WHO standard) |
Vitality (live sperm) | 50% | Greater than 58% |
Round cells | 2million /ml | Less than 5million /ml |
Leucocytes | 0.5million /ml | Less than 1million/ml |
PCD | Primary Ciliary Dysfunction |
DNAI1 | Dynein, Axonemal, Intermediate Chain 1; |
DNAH5 | Dynein, AXonemal, Heavy Chain 5 |
KS | Kartagener’s Syndrome |
CCDC39 | Coiled-Coil Domain-Containing Protein 39 |
CT | Computed Tomography |
FEV1 | Forced Expiratory Volume in 1 Second |
FVC | Forced Vital Capacity |
| [1] | Tadesse A, Alemu H, Silamsaw M, Gebrewold Y. Kartagener’s syndrome: a case report. J Med Case Reports. 2018 Jan 10; 12: 5. |
| [2] | Ciancio N, De Santi MM, Campisi R, Amato L, Di Martino G, Di Maria G. Kartagener’s syndrome: review of a case series. Multidiscip Respir Med. 2015 Dec; 10(1): 18. |
| [3] | Poudel S, Basnet A, Bista S, Shah R, Chhetri BT. Kartagener’s syndrome with recurrent respiratory infection: a case report. Ann Med Surg. 2023 May 10; 85(6): 3102–5. |
| [4] | Kaza S, Fulmali DG. Kartagener’s Syndrome: A Narrative Review on its Clinical Implications and Management. J Clin Diagn Res [Internet]. 2024 [cited 2025 Oct 24]; Available from: |
| [5] | Skeik N, Jabr FI. Kartagener syndrome. Int J Gen Med. 2011 Jan 12; 4: 41–3. |
| [6] | Lwal Y, Suwaid AM, Yahiza MA, et al. Kartagener’s Syndrome in a Young Female: A Rare Diagnosis in a Resource-Limited Facility. West Afr J Radiol 2021; 28: 27-30. |
| [7] | Kartagener M. Zur Pathogenese der bronchiectasien. I Mitteilung: Bronchiectasien being situs viscerum inversus. Betr Klin Tuberk 1933; 83: 498-501. |
| [8] | Bent JP, Smith RJ. Intraoperative diagnosis of primary ciliary dyskinesia. Otolaryngol Head Neck surgery 1997; 116: 64-7. ished: 17 May 2016 |
| [9] | Sarah FI, Hussain MM, Showkat HI, Sarmast AH, Dar NA, Bhat GM. Photoclinic. Kartagener's syndrome, Arch Iran Med 2013; 16: 129-30 9-130 |
| [10] | Sha Y, Ding L, Li P. Management of Primary Ciliary Dyskinesia/Kartagener’s Syndrome in Infertile Male Partners and Current Progress in Defining the Underlying Genetic Mechanism. Asian Journal of Andrology 2014; 16: 101-106., |
| [11] | Chernick V, Boat TF, Wilmont RW, Bush A. Kendig's disorder s of the respiratory tract in children. 7th ed. Philadelphia, PA. Saunders- Elsevier, 2006. P.485-90. |
| [12] | Corbo GM, Foresi A, Bonfitto P, Mugnano A, Agabiti N, Cole PJ. Measurement of nasal mucociliary clearance. Arch Dis Child 1989; 64: 546-50. |
| [13] | Lobo LJ, Zariwala MA, Noone PG. Ciliary dyskinesia: primary ciliary dyskinesia in adults. Eur Respir Mon. 2011; 52: 130-49. |
| [14] | Fraser RS, Muller NL, Colman N, Pare PD. Bronchiectasis and other bronchial abnormalities. In: Fraser RS, Muller NL, Colman N, Pare PD, editors. Diagnosis of diseases of the chest. 4th ed. Philadelphia: WB. Saunders company; 1999.p.2281-3. |
| [15] | Jayashankar CA, Somasekar DS, Perugu PK, Reddy KV, Prakash B, Santosh KV. Kartagener's syndrome: A case report. Such Med case Rep. 2014; 2(1): 7-10. |
APA Style
Ahamefule, O. C., Ekele, R. A., Progress, O., Jafaru, M., Ugwunze, C., et al. (2025). A Case Report of Kartagener’s Syndrome: Clinical Presentation, Diagnosis, and Management Challenges. Central African Journal of Public Health, 11(6), 381-384. https://doi.org/10.11648/j.cajph.20251106.16
ACS Style
Ahamefule, O. C.; Ekele, R. A.; Progress, O.; Jafaru, M.; Ugwunze, C., et al. A Case Report of Kartagener’s Syndrome: Clinical Presentation, Diagnosis, and Management Challenges. Cent. Afr. J. Public Health 2025, 11(6), 381-384. doi: 10.11648/j.cajph.20251106.16
AMA Style
Ahamefule OC, Ekele RA, Progress O, Jafaru M, Ugwunze C, et al. A Case Report of Kartagener’s Syndrome: Clinical Presentation, Diagnosis, and Management Challenges. Cent Afr J Public Health. 2025;11(6):381-384. doi: 10.11648/j.cajph.20251106.16
@article{10.11648/j.cajph.20251106.16,
author = {Ordu Collins Ahamefule and Robert Amadi Ekele and Obdinma-Igwe Progress and Momodu Jafaru and Charles Ugwunze and Ezeifeh Victor Tochukwu and Obazee Emmanuel and Ogbamba Success and Iwuanyanwu-Patrick Chinyere},
title = {A Case Report of Kartagener’s Syndrome: Clinical Presentation, Diagnosis, and Management Challenges
},
journal = {Central African Journal of Public Health},
volume = {11},
number = {6},
pages = {381-384},
doi = {10.11648/j.cajph.20251106.16},
url = {https://doi.org/10.11648/j.cajph.20251106.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20251106.16},
abstract = {Background: Kartagener’s Syndrome (KS) is a rare autosomal recessive genetic disorder characterized by defects in the structure and function of cilia. It is a subset of primary ciliary dyskinesia (PCD) and is defined by a triad of chronic sinusitis, bronchiectasis, and situs inversus totalis. The condition often leads to infertility due to impaired sperm motility. Given its rarity and overlapping symptoms with other respiratory diseases, KS is frequently misdiagnosed. Case Presentation: Our client was a 40-year-old male who presented to the Rivers State University Teaching Hospital, Port Harcourt, Rivers State, South-south Nigeria with recurrent productive cough, rhinorrhea, exertional breathlessness, and wheezing—symptoms have been present since childhood. He had been managed for bronchial asthma at a peripheral center and also reported a history of primary infertility for six years. Clinical examination revealed respiratory distress, oxygen saturation of 87% on room air, and auscultatory findings of coarse crepitations and inspiratory rhonchi. Notably, cardiac auscultation localized heart sounds to the right side of the chest, raising suspicion of situs inversus. A chest computed tomography (CT) scan confirmed cystic bronchiectasis and situs inversus totalis, leading to a diagnosis of Kartagener’s Syndrome. Spirometry demonstrated an obstuctive ventilatory pattern with significantly reduced Forced Expiratory Volume in 1 second (FEV1), Forced Vital Capacity (FVC) and FEV1/FVC ratios. The patient was managed with antibiotics, bronchodilators, steroids, antihistamines, and chest physiotherapy. Educating and counseling the patient on disease condition, referred to psychotherapists/ Social support group. He remains under follow-up in the respiratory clinic for long-term care. Conclusion Kartagener’s Syndrome, though rare, has been reported globally (1–5). Due to symptom overlap with asthma and other chronic respiratory conditions, it is frequently underdiagnosed. Early recognition using clinical evaluation and imaging studies is crucial for appropriate management and improved patient outcomes.
},
year = {2025}
}
TY - JOUR T1 - A Case Report of Kartagener’s Syndrome: Clinical Presentation, Diagnosis, and Management Challenges AU - Ordu Collins Ahamefule AU - Robert Amadi Ekele AU - Obdinma-Igwe Progress AU - Momodu Jafaru AU - Charles Ugwunze AU - Ezeifeh Victor Tochukwu AU - Obazee Emmanuel AU - Ogbamba Success AU - Iwuanyanwu-Patrick Chinyere Y1 - 2025/11/22 PY - 2025 N1 - https://doi.org/10.11648/j.cajph.20251106.16 DO - 10.11648/j.cajph.20251106.16 T2 - Central African Journal of Public Health JF - Central African Journal of Public Health JO - Central African Journal of Public Health SP - 381 EP - 384 PB - Science Publishing Group SN - 2575-5781 UR - https://doi.org/10.11648/j.cajph.20251106.16 AB - Background: Kartagener’s Syndrome (KS) is a rare autosomal recessive genetic disorder characterized by defects in the structure and function of cilia. It is a subset of primary ciliary dyskinesia (PCD) and is defined by a triad of chronic sinusitis, bronchiectasis, and situs inversus totalis. The condition often leads to infertility due to impaired sperm motility. Given its rarity and overlapping symptoms with other respiratory diseases, KS is frequently misdiagnosed. Case Presentation: Our client was a 40-year-old male who presented to the Rivers State University Teaching Hospital, Port Harcourt, Rivers State, South-south Nigeria with recurrent productive cough, rhinorrhea, exertional breathlessness, and wheezing—symptoms have been present since childhood. He had been managed for bronchial asthma at a peripheral center and also reported a history of primary infertility for six years. Clinical examination revealed respiratory distress, oxygen saturation of 87% on room air, and auscultatory findings of coarse crepitations and inspiratory rhonchi. Notably, cardiac auscultation localized heart sounds to the right side of the chest, raising suspicion of situs inversus. A chest computed tomography (CT) scan confirmed cystic bronchiectasis and situs inversus totalis, leading to a diagnosis of Kartagener’s Syndrome. Spirometry demonstrated an obstuctive ventilatory pattern with significantly reduced Forced Expiratory Volume in 1 second (FEV1), Forced Vital Capacity (FVC) and FEV1/FVC ratios. The patient was managed with antibiotics, bronchodilators, steroids, antihistamines, and chest physiotherapy. Educating and counseling the patient on disease condition, referred to psychotherapists/ Social support group. He remains under follow-up in the respiratory clinic for long-term care. Conclusion Kartagener’s Syndrome, though rare, has been reported globally (1–5). Due to symptom overlap with asthma and other chronic respiratory conditions, it is frequently underdiagnosed. Early recognition using clinical evaluation and imaging studies is crucial for appropriate management and improved patient outcomes. VL - 11 IS - 6 ER -
Department of Internal Medicine, University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria
Department of Internal Medicine, University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria