Abstract
BACKGROUND: Chronic kidney disease (CKD) is a major global health concern, often complicated by pulmonary dysfunction. As cardiorespiratory dysfunction progresses, respiratory symptoms in CKD patients may also reflect this. In this study, respiratory symptoms in pre-dialysis CKD patients in southeast Nigeria were evaluated for prevalence and clinical correlations. A total of 240 participants—120 pre-dialysis CKD patients and 120 matched controls—were assessed in this hospital-based cross-sectional investigation. The St. George's Respiratory Questionnaire were used to gather sociodemographic, and clinical data. Respiratory symptoms were compared across stages of chronic kidney disease. Multivariate logistic regression was used to examine relationships between clinical factors and pulmonary function. The results indicated that, there was a substantial increase in respiratory symptoms among CKD patients (60%) compared to controls (11.7%) (OR = 10.5; 95% CI: 5.47-20.17; p < 0.001). The most frequent symptoms were cough (40%) and dyspnea (31.7%). Respiratory symptoms were associated with anemia, edema, and prolonged disease duration. It was concluded that; as CKD progresses, respiratory symptoms and pulmonary dysfunction become more severe. The treatment of CKD prior to dialysis should include routine respiratory evaluations, such as spirometry and symptom monitoring. It takes a multidisciplinary management approach to reduce respiratory morbidity and enhance clinical results.
Keywords
Nigeria, South-east, Spirometry, Pre-dialysis, Respiratory Symptoms, Chronic Kidney Disease, And Pulmonary Function
1. Introduction
Chronic kidney disease (CKD) is diagnosed as a result of screening of people known to be at risk of kidney disease, such as those with high blood pressure or diabetes mellitus, and those with a blood relative with CKD.
| [1] | Bello AK, Alrukhaimi M, Ashuntantang GE, Basnet S, Rotter RC, Douthat WG, et al. Complications of chronic kidney disease: current state, knowledge gaps, and strategy for action. Kidney Int Suppl. 2017; 7(2): 122-9. |
[1]
CKD may also be identified when it leads to one of its recognized complications, such as cardiovascular disease, anemia, pulmonary edema, pleural effusion, pericarditis, and renal osteodystrophy. CKD is an internationally recognized public health problem affecting 5-10% of the world population.
| [2] | Group KDIGO (KDIGO) CMW. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2009; (113): S1-130. |
[2]
There is evidence that its treatment can prevent or delay the progression, reduce or prevent the development of complications, and reduce the risk of cardiovascular and respiratory diseases
| [2] | Group KDIGO (KDIGO) CMW. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2009; (113): S1-130. |
[2]
.
Respiratory symptoms such as dyspnea are the most common of all symptoms associated with Chronic Kidney Disease (CKD).
| [2] | Group KDIGO (KDIGO) CMW. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2009; (113): S1-130. |
[2]
Respiratory diseases were reported as the third leading cause of hospitalization in Canada and the fourth leading cause of disability in the United State of America (USA).
In Nigeria, the work done by Akanbi et al on the burden of respiratory disease in Nigeria showed that respiratory infections, particularly TB and bacterial pneumonia, are the major causes of death in adults and children, with morbidity and mortality due to these diseases rising sharply in HIV-infected persons.
| [4] | Akanbi MO, Ukoli CO, Erhabor GE, Akanbi FO, Gordon SB. The burden of respiratory disease in Nigeria. 2009; |
[4]
Some respiratory symptoms like nasal congestion, anosmia, sneezing, rhinitis, facial pains, sore throat, nosebleed etc., which are suggestive of upper respiratory tract infections while Nocturnal cough, wheeze, breathlessness etc., are suggestive of obstructive airway pattern. Snoring, nocturnal apnea increased daytime somnolence etc., suggestive of obstructive sleep apnea syndrome. Exertional breathlessness, dry cough etc., are suggestive of restrictive airway disease. Chest pain, fever, cough, sputum production, hemoptysis, trepnea are suggestive of lower respiratory tract infection.
The American Academy of Allergy, Asthma and Immunology (AAAAI) defines pulmonary function test as what determines how the lung functions by measuring the amount of air the lungs hold and how fast the air enters and exists the respiratory system. Pulmonary function testing (Spirometry) can be used to diagnose many lung conditions, and its severity can also be suggested by the presence of some respiratory symptoms.
The symptoms of worsening kidney function are not specific and might include feeling generally unwell and experiencing a reduced appetite. Often, chronic kidney disease is diagnosed as a result of screening of people known to be at risk of kidney disease, such as those with high blood pressure or diabetes mellitus and those with a blood relative with CKD. CKD may also be identified when it leads to one of its recognized complications, such as cardiovascular disease, anemia, pulmonary edema, pleural effusion, pericarditis, renal osteodystrophy etc. CKD is an internationally recognized public health problem affecting 5-10% of the world population.
| [2] | Group KDIGO (KDIGO) CMW. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2009; (113): S1-130. |
[2]
There is evidence that its treatment can prevent or delay the progression, reduce or prevent the development of complications, and reduce the risk of cardiovascular and respiratory diseases.
| [2] | Group KDIGO (KDIGO) CMW. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2009; (113): S1-130. |
[2]
CKD cases are nearly always diagnosed clinically, based on severe respiratory symptoms.
| [5] | Basnayake TL, Morgan LC, Chang AB. The global burden of respiratory infections in indigenous children and adults: A review. Respirology. 2017 Nov; 22(8): 1518-28. |
[5]
The burden of respiratory diseases on the populace has been reported to be high, as respiratory diseases appear as one of the major causes of morbidity and mortality among adults and children worldwide.
| [4] | Akanbi MO, Ukoli CO, Erhabor GE, Akanbi FO, Gordon SB. The burden of respiratory disease in Nigeria. 2009; |
[4]
Populations in Asia and Africa bear a significant portion of the burden, with 134 and 131 million cases of lower respiratory infections reported each year, respectively, out of a global total of 429.2 million cases for all ages.
| [6] | Mehta S, Shin H, Burnett R, North T, Cohen AJ. Ambient particulate air pollution and acute lower respiratory infections: a systematic review and implications for estimating the global burden of disease. Air Qual Atmosphere Health. 2013 Mar 1; 6(1): 69-83. |
[6]
Respiratory disorders for 17.4% of all fatalities and 13.3% of all Disability-Adjusted Life Years (DALYs).
| [5] | Basnayake TL, Morgan LC, Chang AB. The global burden of respiratory infections in indigenous children and adults: A review. Respirology. 2017 Nov; 22(8): 1518-28. |
| [7] | Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017 Sep; 5(9): 691-706. |
[5, 7]
In Nigeria and other African countries, chronic kidney disease (CKD) is a prevalent cause of death in hospital wards. Cardiovascular disease is a leading source of morbidity and death in Nigeria and across Africa.
| [8] | Onodugo O, Arodiwe E, Okoye J, Ezeala B, Onodugo N, Ulasi I, et al. Prevalence of autonomic dysfunction among pre-dialysis chronic kidney disease patients in a tertiary hospital, South East Nigeria. Afr Health Sci. 2018 Nov 29; 18(4): 940. |
[8]
The pathogenesis of cardiovascular disease (CVD) in CKD patients remains unknown. Hypertension, diabetes, and hyperlipidemia are well-known risk factors.
| [1] | Bello AK, Alrukhaimi M, Ashuntantang GE, Basnet S, Rotter RC, Douthat WG, et al. Complications of chronic kidney disease: current state, knowledge gaps, and strategy for action. Kidney Int Suppl. 2017; 7(2): 122-9. |
[1]
Chronic kidney disease rarely manifests in isolation, without additional comorbidities. Beyond the common CKD-associated complications, lung diseases can have profound negative effects on kidney function, especially in the presence of other comorbidities, and correlate independently with increased mortality in patients with CKD.
| [9] | Bollenbecker S, Czaya B, Gutiérrez OM, Krick S. Lung-kidney interactions and their role in chronic kidney disease-associated pulmonary diseases. Am J Physiol-Lung Cell Mol Physiol. 2022 May 1; 322(5): L625-40. |
[9]
Chronic kidney disease comorbidities increase the mortality rate, increase the course of the illness, and increase the need for dialysis.
| [10] | Gembillo G, Calimeri S, Tranchida V, Silipigni S, Vella D, Ferrara D, et al. Lung dysfunction and chronic kidney disease: a complex network of multiple interactions. J Pers Med. 2023; 13(2): 286. |
[10]
Complications such as respiratory symptoms have now been identified as contributors to the increased CVD in patients with CKD4.
| [10] | Gembillo G, Calimeri S, Tranchida V, Silipigni S, Vella D, Ferrara D, et al. Lung dysfunction and chronic kidney disease: a complex network of multiple interactions. J Pers Med. 2023; 13(2): 286. |
[10]
There is an obvious overlap between the kidneys and lungs in terms of pH balance, phosphate metabolism, and immune system modulation, even though diabetes and cardiovascular disorders are the conditions that most frequently accompany chronic renal disease. There is a gap in the precise underlying pathways that lead to respiratory symptoms associated with chronic renal disease.
| [9] | Bollenbecker S, Czaya B, Gutiérrez OM, Krick S. Lung-kidney interactions and their role in chronic kidney disease-associated pulmonary diseases. Am J Physiol-Lung Cell Mol Physiol. 2022 May 1; 322(5): L625-40. |
[9]
2. Methods
The Nephrology Clinic at Nnamdi Azikiwe University Teaching Hospital, Nnewi, a tertiary healthcare facility in southeast Nigeria, served as the site of this cross-sectional, analytical hospital-based study. Pre-dialysis adults with chronic kidney disease (CKD stages 1-4) who were enrolled in the nephrology outpatient clinic were included in the study population. The control group consisted of age-matched people who showed no signs of CKD.
Inclusion Criteria:
1) Adults (≥18 years) with confirmed CKD not yet on dialysis.
2) Consenting patients and controls.
Exclusion Criteria:
1) Patients with acute kidney injury or on dialysis.
2) Individuals with known pulmonary diseases or recent respiratory infections.
Data on quality of life and respiratory symptoms were gathered using a modified version of the St. George's Respiratory Questionnaire (SGRQ). After obtaining informed consent from each participant, this was administered.
A portable creatinine analyzer, which yields fast findings (within 30 seconds), was used to quantify the levels of creatinine using finger-prick blood samples taken on 1.2 µL test strips. The creatinine measuring range of the instrument is 0.3-12.0 mg/dL (27-1056 µmol/L).
The U Kidney GFR Calculator was used to determine the estimated glomerular filtration rate (eGFR), which was derived from the condensed MDRD equation:
eGFR = 186 × (Creatinine/88.4)−1.154× (Age)−0.203× (0.742 if female) × (1.210 if Black)
This helped classify patients by CKD stage and exclude controls with reduced kidney function. Before testing, anthropometric measurements (weight and height) and demographic information were collected, patients were fitted with disposable nose clips, and any restrictive clothing or loose dentures were carefully undone.
SPSS version 21.0 was used to analyze the data. For continuous variables, descriptive statistics were presented as means ± standard deviation; for categorical variables, they were presented as frequencies and percentages. The student’s t-test was used to compare continuous variables. Where appropriate, Fisher's exact test or the Chi-square test were used to compare categorical variables. When comparing means across more than two groups, ANOVA was employed. To find variables that are independently linked to respiratory symptoms in patients with chronic kidney disease, multivariate logistic regression was used. The model included variables that were significant in univariate analysis. 95% Confidence Intervals (CI) and Adjusted Odds Ratios (OR) were shown. Statistical significance was defined as a p-value of less than 0.05.
The Research Ethics Committee of Nnamdi Azikiwe University Teaching Hospital in Nnewi provided ethical approval. In compliance with the Declaration of Helsinki, the study was carried out. Written consent was obtained and data was kept anonymous.
3. Results
3.1. Sociodemographic and Clinical Characteristics
The study had 240 participants—120 pre-dialysis chronic kidney disease patients and 120 matched healthy controls. The male-to-female ratio was roughly 1.2:1, and the mean ages of the two groups were comparable. The majority of CKD patients were in advanced stages: 70% in stage 4 and 96.9% in stage 5, signifying late presentation. The prevalence of smoking history was greater in CKD patients (7.5%) than in controls (0.8%). Notably specific data for anemia and edema were absent, both diseases were common and likely exacerbated the respiratory symptoms noted in the CKD cohort.
Table 1. Baseline Characteristics of Study Participants.
Variable | CKD Patients (n=120) | Controls (n=120) | p-value |
Age (years) | 52.6 ± 11.8 | 50.9 ± 10.5 | 0.256 |
Male: Female | 66: 54 | 60: 60 | 0.431 |
Smoker (%) | 9 (7.5%) | 1 (0.8%) | 0.017* |
Edema (%) | 85 (70.8%) | 0 (0%) | <0.001* |
Anemia (%) | 92 (76.7%) | 4 (3.3%) | <0.001* |
3.2. Prevalence and Pattern of Respiratory Symptoms
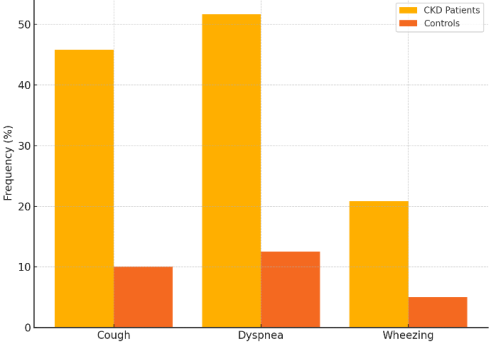
Compared to controls, respiratory symptoms were significantly more common in CKD patients. Only 14 controls (11.7%) reported any respiratory symptoms, but 72 CKD patients (60.0%) reported at least one (χ² = 58.580; p < 0.0001). CKD patients were 10.5 times more likely than controls to experience respiratory symptoms (OR = 10.5; 95% CI: 5.47-20.17). Cough (47.5%) and dyspnea (30.2%) were the most often reported symptoms among CKD patients, and both were substantially more common than in controls (p < 0.001). Wheezing was not present in controls, although it was recorded in 8.3% of CKD patients. With 5.8% of CKD patients and 4.2% of controls experiencing sputum production, it was the least common symptom with no statistically significant difference (p = 0.554).
Table 2. Prevalence of Respiratory Symptoms Among Study Participants.
Symptom | CKD Patients (%) (n=120) | Controls (%) (n=120) | p-value |
Cough | 48 (40.0%) | 11 (9.2%) | <0.001* |
Dyspnea | 38 (31.7%) | 4 (3.3%) | <0.001* |
Wheezing | 17 (14.2%) | 2 (1.7%) | 0.001* |
Figure 1. Symptom frequency in CKD patient vs Controls.
4. Discussion
According to this study, respiratory symptoms were found in 60% of pre-dialysis CKD patients, compared to just 12.5% of matched controls. Similar symptom patterns, with cough (~40%) and dyspnea (~39%) being the most prevalent manifestations, are found in Nepal (61.8%).
| [11] | Pant P, Baniya S, Jha A. Prevalence of Respiratory Manifestations in Chronic Kidney Diseases; A Descriptive Cross-sectional Study in a Tertiary Care Hospital of Nepal. JNMA J Nepal Med Assoc. 2019 Apr; 57(216): 80-3. |
[11]
As CKD progresses, respiratory symptoms develop significantly (from 15.8% in stage 3 to 96.9% in stage 5). This indicates that renal impairment has a gradual effect on pulmonary health. Fluid overload, uremic endothelial dysfunction, hypoalbuminemia, and cardiovascular comorbidities are significant contributors to pulmonary problems in chronic kidney disease (CKD), according to previous research.
| [12] | Parivakkam Mani A, K S, Sundar R, Yadav S. Pulmonary Manifestations at Different Stages in the Chronic Kidney Disease: An Observational Study. Cureus. 15(5): e39235. |
| [13] | Sharma A, Sharma A, Gahlot S, Prasher PK. A study of pulmonary function in end-stage renal disease patients on hemodialysis: a cross-sectional study. São Paulo Med J. 2017 Sep 28; 135(6): 568-72. |
[12, 13]
Furthermore, extensive cohort studies demonstrate that restrictive lung dysfunction is independently linked to mortality risks and is becoming more common in advanced chronic kidney disease: Patients who had decreased lung function and respiratory symptoms had greater cardiovascular and all-cause death rates.
| [10] | Gembillo G, Calimeri S, Tranchida V, Silipigni S, Vella D, Ferrara D, et al. Lung dysfunction and chronic kidney disease: a complex network of multiple interactions. J Pers Med. 2023; 13(2): 286. |
| [11] | Pant P, Baniya S, Jha A. Prevalence of Respiratory Manifestations in Chronic Kidney Diseases; A Descriptive Cross-sectional Study in a Tertiary Care Hospital of Nepal. JNMA J Nepal Med Assoc. 2019 Apr; 57(216): 80-3. |
| [13] | Sharma A, Sharma A, Gahlot S, Prasher PK. A study of pulmonary function in end-stage renal disease patients on hemodialysis: a cross-sectional study. São Paulo Med J. 2017 Sep 28; 135(6): 568-72. |
| [14] | Mukai H, Ming P, Lindholm B, Heimbürger O, Barany P, Stenvinkel P, et al. Lung Dysfunction and Mortality in Patients with Chronic Kidney Disease. Kidney Blood Press Res. 2018; 43(2): 522-35. |
| [15] | Anees M, Akbar H, Ibrahim M, Saeed MS, Ismail M. Pulmonary Functions and Factors Affecting Them in Patients with Chronic Kidney Disease. J Coll Physicians Surg--Pak JCPSP. 2020 Oct; 30(10): 1082-5. |
[10, 11, 13-15]
Cough and dyspnea were respiratory symptoms that were substantially linked to worse clinical results. The length of CKD and its advanced stage were similarly associated with declining lung function, which supports eGFR's validity as a reliable indicator of respiratory impairment.
According to earlier research, anemia and falling GFR are the main risk factors for pulmonary dysfunction in CKD patients.
| [15] | Anees M, Akbar H, Ibrahim M, Saeed MS, Ismail M. Pulmonary Functions and Factors Affecting Them in Patients with Chronic Kidney Disease. J Coll Physicians Surg--Pak JCPSP. 2020 Oct; 30(10): 1082-5. |
[15]
The significant prevalence of anemia and probable fluid overload (e.g., edema) in our group undoubtedly contributed to the burden of symptoms, even though specific Hb data was not defined. A known risk factor for chronic respiratory symptoms in Southeastern Nigeria is high ambient air pollution (PM
2.5 levels averaging >70 μg/m
3), which may worsen impairment in individuals with chronic kidney disease
The reported respiratory effects are probably exacerbated by this environmental burden, while more information on exposure levels would assist to elucidate this connection.
Numerous processes could account for the pulmonary impairment that has been observed; an excess of fluid that results in interstitial pulmonary edema, capillary leakage is encouraged and oncotic pressure is decreased by hypoalbuminemia, reduced lung compliance and pulmonary hypertension are caused by uremic toxins and endothelial dysfunction (12, 15, 17) and in CKD, inflammation-malnutrition complex syndrome (MICS) is prevalent and is associated with increased morbidity and decreased lung function.(12, 13, 15) These findings underscore the need for routine respiratory screening in CKD clinics—particularly spirometry and symptom assessment. The high odds ratio for respiratory symptoms in CKD (OR ≈ 10.5) suggests early identification and management may reduce morbidity. Pulmonary dysfunction should also trigger evaluation of fluid status, hemoglobin level, and nutritional status.
5. Conclusion
Pre-dialysis patients with chronic kidney disease (CKD) in southeast Nigeria have a notably high incidence of respiratory symptoms, according to this study, and the severity of their symptoms and impairment of their pulmonary function increases with the stage of CKD. The most prevalent symptoms were cough and dyspnea, which were strongly linked to anemia, growing eGFR, prolonged illness duration, and volume overload.
Our results highlight how important it is to identify respiratory symptoms early and do routine pulmonary function assessments as part of CKD care procedures, especially prior to starting dialysis. Nephrologists, pulmonologists, and public health specialists must work together in a multidisciplinary approach because to the complex pathophysiology that includes uremic toxins, fluid retention, anemia, and potential environmental exposures.
The quality of life in this susceptible group may be improved and the risk of respiratory issues reduced by implementing spirometry, monitoring for anemia, managing fluid overload, and enhancing environmental health. To examine the course of pulmonary decline and evaluate the effects of focused therapies, further longitudinal and interventional research is advised.
Author Contributions
Ordu Collins Ahamefule: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing
Ugwuunze Charles: Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing
Ezeifeh Victor Tochukwu: Funding acquisition, Resources, Software, Validation, Visualization, Writing – original draft
Patrick-Iwuanyanwu Chinyere: Data curation, Formal Analysis, Methodology, Resources, Software, Validation, Writing – original draft, Writing – review & editing
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Bello AK, Alrukhaimi M, Ashuntantang GE, Basnet S, Rotter RC, Douthat WG, et al. Complications of chronic kidney disease: current state, knowledge gaps, and strategy for action. Kidney Int Suppl. 2017; 7(2): 122-9.
|
| [2] |
Group KDIGO (KDIGO) CMW. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2009; (113): S1-130.
|
| [3] |
Hubbard R. The burden of lung disease . Vol. 61, Thorax. BMJ Publishing Group Ltd; 2006 [cited 2025 Jun 27]. p. 557-8. Available from:
https://thorax.bmj.com/content/61/7/557.extract
|
| [4] |
Akanbi MO, Ukoli CO, Erhabor GE, Akanbi FO, Gordon SB. The burden of respiratory disease in Nigeria. 2009;
|
| [5] |
Basnayake TL, Morgan LC, Chang AB. The global burden of respiratory infections in indigenous children and adults: A review. Respirology. 2017 Nov; 22(8): 1518-28.
|
| [6] |
Mehta S, Shin H, Burnett R, North T, Cohen AJ. Ambient particulate air pollution and acute lower respiratory infections: a systematic review and implications for estimating the global burden of disease. Air Qual Atmosphere Health. 2013 Mar 1; 6(1): 69-83.
|
| [7] |
Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017 Sep; 5(9): 691-706.
|
| [8] |
Onodugo O, Arodiwe E, Okoye J, Ezeala B, Onodugo N, Ulasi I, et al. Prevalence of autonomic dysfunction among pre-dialysis chronic kidney disease patients in a tertiary hospital, South East Nigeria. Afr Health Sci. 2018 Nov 29; 18(4): 940.
|
| [9] |
Bollenbecker S, Czaya B, Gutiérrez OM, Krick S. Lung-kidney interactions and their role in chronic kidney disease-associated pulmonary diseases. Am J Physiol-Lung Cell Mol Physiol. 2022 May 1; 322(5): L625-40.
|
| [10] |
Gembillo G, Calimeri S, Tranchida V, Silipigni S, Vella D, Ferrara D, et al. Lung dysfunction and chronic kidney disease: a complex network of multiple interactions. J Pers Med. 2023; 13(2): 286.
|
| [11] |
Pant P, Baniya S, Jha A. Prevalence of Respiratory Manifestations in Chronic Kidney Diseases; A Descriptive Cross-sectional Study in a Tertiary Care Hospital of Nepal. JNMA J Nepal Med Assoc. 2019 Apr; 57(216): 80-3.
|
| [12] |
Parivakkam Mani A, K S, Sundar R, Yadav S. Pulmonary Manifestations at Different Stages in the Chronic Kidney Disease: An Observational Study. Cureus. 15(5): e39235.
|
| [13] |
Sharma A, Sharma A, Gahlot S, Prasher PK. A study of pulmonary function in end-stage renal disease patients on hemodialysis: a cross-sectional study. São Paulo Med J. 2017 Sep 28; 135(6): 568-72.
|
| [14] |
Mukai H, Ming P, Lindholm B, Heimbürger O, Barany P, Stenvinkel P, et al. Lung Dysfunction and Mortality in Patients with Chronic Kidney Disease. Kidney Blood Press Res. 2018; 43(2): 522-35.
|
| [15] |
Anees M, Akbar H, Ibrahim M, Saeed MS, Ismail M. Pulmonary Functions and Factors Affecting Them in Patients with Chronic Kidney Disease. J Coll Physicians Surg--Pak JCPSP. 2020 Oct; 30(10): 1082-5.
|
| [16] |
Health in Nigeria. In: Wikipedia . 2025 [cited 2025 Jul 19]. Available from:
https://en.wikipedia.org/w/index.php?title=Health_in_Nigeria&oldid=1301070670
|
| [17] |
Preserved ratio impaired spirometry, airflow obstruction, and their trajectories in relationship to chronic kidney disease: a prospective cohort study - PubMed . [cited 2025 Jul 19]. Available from:
https://pubmed.ncbi.nlm.nih.gov/39870785/
|
Cite This Article
-
APA Style
Ahamefule, O. C., Charles, U., Tochukwu, E. V., Chinyere, P. (2025). Prevalence and Clinical Correlates of Respiratory Symptoms in Pre-Dialysis Patients with Chronic Kidney Disease in a Tertiary Hospital in Southeastern Nigeria. Central African Journal of Public Health, 11(6), 396-400. https://doi.org/10.11648/j.cajph.20251106.18
 Copy
|
Copy
|
 Download
Download
ACS Style
Ahamefule, O. C.; Charles, U.; Tochukwu, E. V.; Chinyere, P. Prevalence and Clinical Correlates of Respiratory Symptoms in Pre-Dialysis Patients with Chronic Kidney Disease in a Tertiary Hospital in Southeastern Nigeria. Cent. Afr. J. Public Health 2025, 11(6), 396-400. doi: 10.11648/j.cajph.20251106.18
Copy
|
Download
AMA Style
Ahamefule OC, Charles U, Tochukwu EV, Chinyere P. Prevalence and Clinical Correlates of Respiratory Symptoms in Pre-Dialysis Patients with Chronic Kidney Disease in a Tertiary Hospital in Southeastern Nigeria. Cent Afr J Public Health. 2025;11(6):396-400. doi: 10.11648/j.cajph.20251106.18
Copy
|
Download
-
@article{10.11648/j.cajph.20251106.18,
author = {Ordu Collins Ahamefule and Ugwuunze Charles and Ezeifeh Victor Tochukwu and Patrick-Iwuanyanwu Chinyere},
title = {Prevalence and Clinical Correlates of Respiratory Symptoms in Pre-Dialysis Patients with Chronic Kidney Disease in a Tertiary Hospital in Southeastern Nigeria},
journal = {Central African Journal of Public Health},
volume = {11},
number = {6},
pages = {396-400},
doi = {10.11648/j.cajph.20251106.18},
url = {https://doi.org/10.11648/j.cajph.20251106.18},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20251106.18},
abstract = {BACKGROUND: Chronic kidney disease (CKD) is a major global health concern, often complicated by pulmonary dysfunction. As cardiorespiratory dysfunction progresses, respiratory symptoms in CKD patients may also reflect this. In this study, respiratory symptoms in pre-dialysis CKD patients in southeast Nigeria were evaluated for prevalence and clinical correlations. A total of 240 participants—120 pre-dialysis CKD patients and 120 matched controls—were assessed in this hospital-based cross-sectional investigation. The St. George's Respiratory Questionnaire were used to gather sociodemographic, and clinical data. Respiratory symptoms were compared across stages of chronic kidney disease. Multivariate logistic regression was used to examine relationships between clinical factors and pulmonary function. The results indicated that, there was a substantial increase in respiratory symptoms among CKD patients (60%) compared to controls (11.7%) (OR = 10.5; 95% CI: 5.47-20.17; p < 0.001). The most frequent symptoms were cough (40%) and dyspnea (31.7%). Respiratory symptoms were associated with anemia, edema, and prolonged disease duration. It was concluded that; as CKD progresses, respiratory symptoms and pulmonary dysfunction become more severe. The treatment of CKD prior to dialysis should include routine respiratory evaluations, such as spirometry and symptom monitoring. It takes a multidisciplinary management approach to reduce respiratory morbidity and enhance clinical results.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Prevalence and Clinical Correlates of Respiratory Symptoms in Pre-Dialysis Patients with Chronic Kidney Disease in a Tertiary Hospital in Southeastern Nigeria
AU - Ordu Collins Ahamefule
AU - Ugwuunze Charles
AU - Ezeifeh Victor Tochukwu
AU - Patrick-Iwuanyanwu Chinyere
Y1 - 2025/12/09
PY - 2025
N1 - https://doi.org/10.11648/j.cajph.20251106.18
DO - 10.11648/j.cajph.20251106.18
T2 - Central African Journal of Public Health
JF - Central African Journal of Public Health
JO - Central African Journal of Public Health
SP - 396
EP - 400
PB - Science Publishing Group
SN - 2575-5781
UR - https://doi.org/10.11648/j.cajph.20251106.18
AB - BACKGROUND: Chronic kidney disease (CKD) is a major global health concern, often complicated by pulmonary dysfunction. As cardiorespiratory dysfunction progresses, respiratory symptoms in CKD patients may also reflect this. In this study, respiratory symptoms in pre-dialysis CKD patients in southeast Nigeria were evaluated for prevalence and clinical correlations. A total of 240 participants—120 pre-dialysis CKD patients and 120 matched controls—were assessed in this hospital-based cross-sectional investigation. The St. George's Respiratory Questionnaire were used to gather sociodemographic, and clinical data. Respiratory symptoms were compared across stages of chronic kidney disease. Multivariate logistic regression was used to examine relationships between clinical factors and pulmonary function. The results indicated that, there was a substantial increase in respiratory symptoms among CKD patients (60%) compared to controls (11.7%) (OR = 10.5; 95% CI: 5.47-20.17; p < 0.001). The most frequent symptoms were cough (40%) and dyspnea (31.7%). Respiratory symptoms were associated with anemia, edema, and prolonged disease duration. It was concluded that; as CKD progresses, respiratory symptoms and pulmonary dysfunction become more severe. The treatment of CKD prior to dialysis should include routine respiratory evaluations, such as spirometry and symptom monitoring. It takes a multidisciplinary management approach to reduce respiratory morbidity and enhance clinical results.
VL - 11
IS - 6
ER -
Copy
|
Download